Recurrent Corneal Erosions
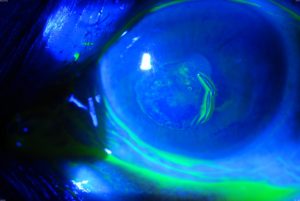
Recurrent corneal erosions are episodes of eye pain due to abnormalities of the surface layer of the cornea (epithelium) that causes it to be poorly adherent to the rest of the cornea.
Call Us: 215-928-3180
 The surface layer of the cornea (epithelium) is supposed to be well attached to the body of the cornea (stroma).
The surface layer of the cornea (epithelium) is supposed to be well attached to the body of the cornea (stroma).
In some eyes, often after trauma to the cornea or in eyes with certain corneal dystrophies (especially epithelial basement membrane dystrophy or EBMD), but occasionally out of the blue, the surface layer separates from the body of the cornea causing pain. The pain may be fleeting or can last for hours or days, depending on how much of the surface layer separates and whether a corneal abrasion occurs.
Recurrent erosions generally respond to medical treatment with antibiotics and lubricants or a bandage soft contact lens. If unsuccessful, a variety of surgeries can be effective ranging from anterior stromal micropuncture, removal of the epithelium with or without diamond burr polishing of the stroma (see “Surgical Procedures” page), to excimer laser resurfacing (phototherapeutic keratectomy or PTK) (see “Surgical Procedures” page).