Symptoms
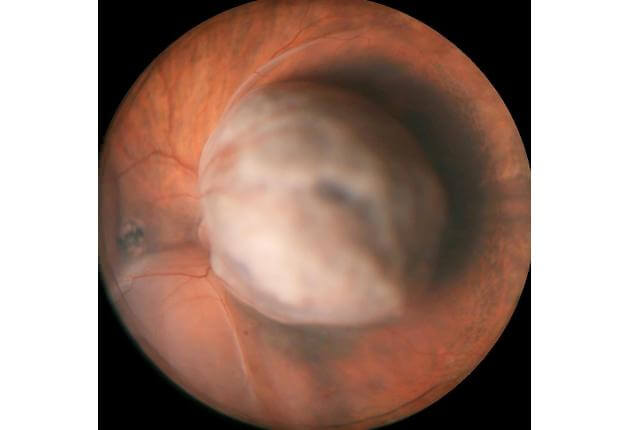
Melanoma can occur in several regions of the eye including the iris, ciliary body, and choroid. These regions are collectively known as the uvea. It typically arises in mid-life in both men and women with no environmental cause, except that it might be more common in arc welders. This tumor can arise from a pre-existent nevus or it can arise de novo, that is without a pre-existing lesion. Melanoma can strike with symptoms of blurred vision, flashing lights, floaters, and rarely pain. Many patients have no symptoms. Melanoma carries a risk for spread (metastasis) to the liver, lung, and skin, so lifelong systemic monitoring is advised. Early treatment of this eye cancer is important to protect from metastasis.
Diagnosis
The diagnosis of uveal melanoma is made by recognition of the typical features of this cancer by an experienced eye doctor using indirect ophthalmoscopy. Ophthalmoscopy is a technique whereby the doctor uses a headset with a light and focuses through the pupil into the back of the eye to visualize the tumor. There are other useful tests that are comfortable and can be performed in the office to confirm melanoma and these include transillumination, ocular ultrasonography, fluorescein angiography, indocyanine green angiography, autofluorescence, ocular coherence tomography and ultrasound biomicroscopy. When the tumor diagnosis remains unclear, fine needle biopsy in the operating room can be used to give an exact diagnosis.
Risk Factors
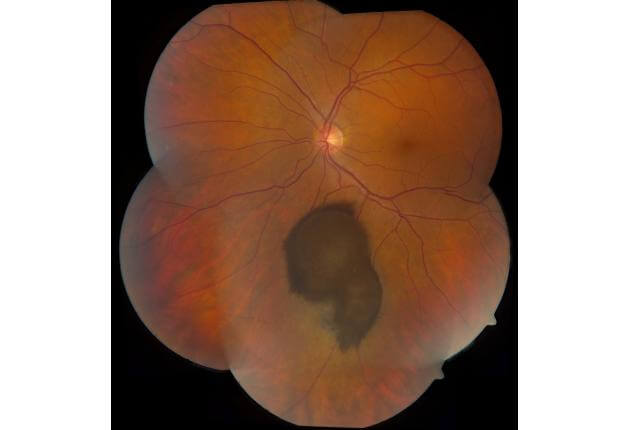
The goal of melanoma management is to detect the tumor early so that metastasis is minimized. When the doctor finds a small borderline tumor that could be a benign nevus or a cancerous melanoma, there are risk factors that have been identified and published by the Oncology Service at Wills Eye Hospital, that serve to identify the small melanoma. These factors include thickness over 2 mm, subretinal fluid, symptoms, orange pigment, tumor margin near the optic disc, lack of chronic drusen, lack of surrounding halo, and hollowness on ultrasonography. These risk factors are critical to judging the malignant potential of a small, pigmented choroidal tumor.
Treatment
There are several treatment methods available for melanoma including:
- Enucleation
- Plaque radiotherapy
- Partial lamellar sclerouvectomy (resection)
- Laser photocoagulation
- Thermotherapy
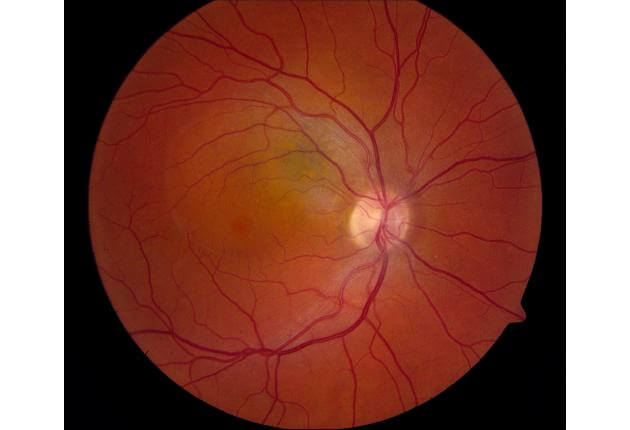
Transpupillary thermotherapy (TTT) can be effective for small tumors away from the optic nerve or center of vision, whereas plaque radiotherapy is used for small, medium and large-size melanomas. The Oncology Service at Wills Eye Hospital has been instrumental in the development and modification of plaque radiotherapy over the past 4 decades. Special custom-designed radioactive plaques have been created so that melanoma at any site in the eye can be feasibly treated and controlled with radiotherapy.
On the Oncology Service, combination treatment for melanoma with plaque radiotherapy followed by TTT provides excellent control in 98% of patients. Only 2% of patients might not be controlled and might need further treatment with other methods. Enucleation is reserved for very large tumors, especially those that have extended outside the wall of the eye or are located around the optic nerve. Even though the melanoma is cured and in remission in the eye, life-long systemic monitoring for metastasis is necessary, as metastasis could have occurred before the eye cancer was discovered. Chemotherapy and immunotherapy regimens (using melanoma vaccine) are used if there is metastasis and they can offer some control.
There is new evidence that genetic mutations can affect the patient prognosis. Many centers require the eye to be removed (enucleation) for genetic testing. The Oncology Service has pioneered the use of fine needle aspiration biopsy for genetic testing. We have found that patients with disomy of chromosome 3 (less aggressive cell type) have a better life prognosis and those with monosomy of chromosome 3 (more aggressive cell type) have a more guarded prognosis and may require additional chemotherapy.